بیماریهای زنان زایمان و نازایی
وب لاگ رسمی دکتر رویا پورقربان جراح و منخصص زنان زایمان و نازایی بورد تخصصی از دانشگاه تهرانبیماریهای زنان زایمان و نازایی
وب لاگ رسمی دکتر رویا پورقربان جراح و منخصص زنان زایمان و نازایی بورد تخصصی از دانشگاه تهراناستفاده از جنین منجمد شده

"انتقال جنین منجمد شده "
............. ادامه مطلب ...........
(MESA) و (PESA) و(TESE)و(TESA)
استخراج اسپرم از بیضه
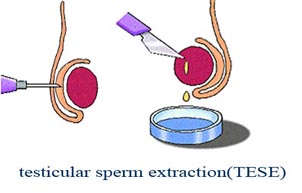
Sperm Extraction:
(MESA) و (PESA) و ( TESE) و(TESA)
جهت عمل ای وی اف و میکرواینجکشن
..............ادامه مطلب.........
انواع روشهای کمک باروری
: انواع روشهای درمان ناباروری (کمک باروری ) ART
به روشهایی که طی آنها تخمک مستقیما از تخمدان برداشته میشود گفته میشود
باروری آزمایشگاهی :IVF : in vitro fertilization
- استخراج تخمک ها – بارور کردن آنها با اسپرم شوهر بیمار در محیط آزمایشگاه و انتقال جنین از طریق دهانه رحم بداخل رحم
- انتقال گامت بداخل لوله فالوپ " گیفت"
GIFT: Gamete intrafallopian Transfer
قرار دادن تخمک و اسپرم در داخل لوله رحم
· انتقال داخل فالوپ جنین: زیفت
ZIFT: Zygote Intrafallopian Transfer
· انتقال لوله ای رویان :
Tubal Embryo Transfer
· انتقال صفاقی تخمک و اسپرم : قرار دادن تخمک و اسپرم در حفره صفاق
· تزریق یک اسپرم واحد در سیتوپلاسم داخل تخمک :ICSI
ICSI: Intracytoplasmic Sperm injection
- خارج ساختن اسپرم از خود بیضه : TESE
TESE: Testicular Sperm Extraction
در مردانی که ازمایش اسپرم آنها " آزواسپرم" یعنی فقدان اسپرم گزارش شده است ولی در نمونه برداری از بافت بیضه آنها میتوان اسپرم را مشاهده نمود و از این اسپرمها میتوان استخراج و جهت انجام ای وی اف استفاده نمود.
- آسپیراسیون اسپرم از اپیدیدیم : MESA
MESA : Microsurgical Epididymal Sperm Aspiration
در کسانی که انسدادی در لوله های منی بر وجود دارد و علیرغم اینکه در ازمایش اسپرم آنها نمومه اسپرم وجود ندارد ولی در لوله های منی بر (اپیدیدیم ) اسپرم وجود دارد و از این اسپرمها برای ای وی اف استفاده میشود
روش انتقال جنین بداخل رحم در ای وی اف
روش انتقال جنین بداخل رحم در عمل ای وی اف
ابتدایی ترین روش برای انتقال جنین روش "Clinical touch " بوده است. در این روش کاتتر انتقال جنین بداخل رحم به آرامی فرو برده میشود تا اینکه نوک آن با فوندوس رحم تماس حاصل نماید سپس آنرا mm 10-5 بیرون کشیده و جنین به آرامی به بیرون رانده میشود.. پیگیری های بعمل آمده در مورد تکنیک انتقال جنین نشان داده است که ایجاد خونریزی رحمی روی جنین اثر توکسیک داشته و تحریک انقباضات رحم نیز تاثیر منفی داشته است لذا تاکید بر انتقال آتروماتیک جنین افزایش یافته است . از آنجائیکه امروزه از تماس با فوندوس رحم اجتناب میشود توصیف "Clinical touch "بشکل استفاده ازروشهای دیگر با اجتناب از تماس با فوندوس تغییر یافته است ولی از ماشینهای اضافی برای تعیین محل نوک کاتتر " سونوگرافی " استفاده نمی شود. روشی که بکار میرود اکثرا روش "blind " است زیرا محل قرار گرفتن نوک کاتتر اثبات نمیگردد و بر اساس احساس سوبژکتیو خود جراح از محل قرار گرفتن کاتتر و یا با توجه به سایر علاین مانند خطوطی که بفواصل مساوی در طول کاتتر قرار دارند و عمق ورود را نشان میدهند عمل انتقال جنین صورت می گیرد .
سونوگرفی بعنوان روش کمکی در انتقال جنین ابتدا در اوایل تجربیات IVF در انسان بکار گرفته شد ولی این جنبه از تکنولوژی کمک باروری مورد علاقه زیادی واقع نشد تا اینکه پیشرفت در سایرجنبه های IVF مانند محیط کشت بعمل آمد در این زمان احتمال اینکه این روش بظاهر بی ضرر میتواند نتایج کلی این مراحل پیچیده را بر هم زند مورد توجه واقع شده بود ولی تلاشی برای استفاده از سونوگرافی در روند انتقال جنین صورت نمی گرفت.اولین مطالعه ای که برای روشن نمودن اثرات سونوگرافی وبیان نکات منفی انتقال جنین به روش "blind" صورت گرفت 12 مورد انتقال جنین به روش "Clinical touch " را با 16 مورد با استفاده ز سونوگرافی ترانس ابدومینال با یکدیگر مقایسه نموده بود .(1) وقتی سونوگرافی انجام می شد کاتتر تا اندازه ای وارد حفره رحم میشد که در سونوگرافی دیده میشد که در اثر تماس با فوندوس رحم خمیده شده است سپس اندکی بیرون کشیده می شد و انتقال جنین صورت می گرفت . در 3 نفر از 16 مورد انتقال جنین که با هداین سونوگرافی صورت میگرفت (8/18%) دیده شد که در زمانی که جراح فکر میکرد کاتتر را درست جایگذاری کرده است نوک کاتتر در مجاورت دیواره خلفی رحم بود و ا و تا زمانیکه با توجه به مشاهدات سونوگرافی به او هشدار داده شد از محل نامناسب کاتتر بی اطلاع بود. این یافته نشان داد که شواهد کلینیکی برای تعیین محل کاتتر ممکنست کافی نباشند.
روش انتقال جنین بکمک سونوگرافی از نظر سوبژکتیو آسان بود و میتواند از "operator bias" جلوگیری کرده باشد . میزان خون با اسیب دیدگی با کاتتر نیز کمتر بود . مولفین اشاره کردند که با توجه به تعداد کم بیمارانی که وارد مطالعه شده بودند انها دلایل آماری برای اثبات اینکه این روش انتقال جنین بهتر است ندارند ولی بیان کردند که در این زمینه تحقیقات بیشتری مورد نیاز می باشد.
غیر قابل اعتماد بودن روش سنتی انتقال جنین در یک مطالعه دیگر نیز که بکمک سونوگرافی واژینال انجام شده بود نشان داده شد.این مطالعه نشان داد که از میان 121 مورد پی در پی انتقال جنین در 4/17% موارد نوک کاتتر در مجاورت فوندوس و در 4/7% در مجاورت لوله بوده است. (2) گاهی برای جاگذاری کاتتر نیاز به مانیپولاسیونهای زیادی می باشد و شاید خارج نمودن اسپیکولوم و گذاشتن پروب واژینال نقشی در جاگذاری نهایی کاتتر داشته باشداگر چه معمولا پزشک از محل قرار گرفتن کاتتر نسبت به لند مارکهای آناتومیک بی اطلاع است .
ادامه مطلب.......
ترجمه از دکتر رویا پورقربان
ادامه مطلب ...روش برداشتن تخمک در ای وی اف
روش برداشتن تخمک در جریان عمل ای وی اف
برداشتن تخمک در عمل ای وی اف بکمک سونوگرافی انجام میگیرد روش این عمل در
زیر به تفضیل مورد بحث و بررسی قرار میگیرد
ادامه مطلب.........
ادامه مطلب ...اصول باروری -انجماد اسپرم -انجماد جنین -انجماد تخمک -پیوند تخمدا
اصول باروری
انجماد اسپرم
انجماد جنین
انجماد تخمک
پیوند تخمدان
ادامه مطلب ...Laser zona pellucida thinning 'ineffective'
طبق اخرین مقالات عمل Laser zona pellucida thinning ' که برای بهتر شدن
احتمال لانه گزینی جنین در اعمال ای وی اف ومیکرواینجکشن بعمل میاید تاثیر زیادی در
بهبود بخشیدن به میزان لانه گزینی نداشته است .
Source: Fertility and Sterility 2008; Advance online publication
اصل مقاله در ادامه مطلب :
ادامه مطلب ...زن 59 ساله فرانسوی 3 قلو زایید
زن 59 ساله فرانسوی 3 قلو زایید |
| 2008/09/10 |
فارس: زن 59 ساله فرانسوی در بیمارستانی در پاریس از طریق عمل سزارین 3 قلو زایید که حال همه فرزندان وی خوب است. |
ای وی اف و میکرواینجکشن
In Vitro Fertilization (IVF) & Assisted Reproduction Techniques (ART)
Ruth Lathi, MD
Clinical Assistant Professor
Department of OB/GYN
Division of Reproductive Endocrinology and Infertility
Barry Behr, PhD, HCLD
Director of IVF/ART and Andrology Laboratories
Stanford University Medical Center
Associate Professor of OB/GYN, & Board Certified Laboratory Director (HCLD)
IVF is a procedure which involves fertilizing eggs and growing the fertilized eggs, outside of the body in a laboratory, then placing the fertilized egg (embryo) in the uterus, in order to achieve a pregnancy. It is a commonly used treatment, to help couples with infertility achieve pregnancy. In this overview, we will discuss the process of IVF from patient evaluation to production and fertilization of the eggs, to selection of embryos to transfer. Pregnancy rates and variation of standard IVF will be addressed in the frequently asked questions section at the end.
The first step is evaluating the cause of infertility with a set of basic tests such as follicle stimulating hormone (FSH) level, hysterosalpingogram (HSG), and semen analysis). These tests will give many couples an idea of their cause of infertility. In the setting of unexplained infertility, couples have the option of performing a laparoscopy to evaluate and treat endometriosis or proceeding with empiric fertility treatments, not knowing the cause. For some patients, IVF is their only realistic option of conceiving a child. Patients with bilateral fallopian tube obstruction or severe male factor infertility have very low odds of conceiving naturally or with simpler fertility treatments and therefore encouraged to proceed directly to IVF. Patients failing other treatments or who are over 40 may also elect to proceed to IVF treatment for infertility, for a better chance of conceiving.

When the eggs are retrieved they are surrounded by supporting cells called cumulus cells.
There are several components to the IVF procedure. The first step involves producing the eggs with a combination of ovarian stimulation and oocyte retrieval. Because not every egg will fertilize and develop normally, medications are used to stimulate the production of multiple eggs in order to boost the odds of success per cycle. The medication protocol used will depend on patient characteristics but will typically use injectable FSH alone or in combination with other hormonal treatments. The medications are given by daily subcutaneous (under the skin) injections. The ovarian response is monitored by ultrasound and blood hormone levels. When the ovaries appear to have enough mature eggs, the physician will perform the oocyte retrieval. The eggs are removed using the assistance of transvaginal ultrasound and suction though a needle that passes through the top of the vagina into the ovary and all mature follicles are aspirated. This procedure is typically performed using conscious sedation or monitored anesthesia care, to ensure that the woman is comfortable.

Intracytoplasmic sperm injection (ICSI) is a procedure where a single sperm is injected into the center of a mature egg.
The method of fertilizing the eggs depends on the quality of the sperm and a couple’s prior experience with IVF. There are two methods commonly used; insemination and intracytoplasmic sperm injection (ICSI). Insemination is a process of washing the sperm and putting a measured concentration of good quality sperm with the eggs and waiting. This method allows the sperm to contact and penetrate the egg more naturally. However it requires at least 5-10 million motile sperm to be most effective. With good sperm and egg quality we expect 60-70% of the eggs to fertilize normally. If the sperm quality or quantity is low then fertilization rates with insemination are lower and ICSI is recommended. This is a procedure involves injecting a single sperm into the middle of the egg, using a micropipette. Despite the fact that many of the natural processes required for normal fertilization are bypassed using this method, the fertilization rates, embryo development and pregnancy rates are similar to standard IVF, when insemination is used. A fertilized egg is now called an embryo.

The fertilized egg has 2 pronuclei. This is the first sign of fertilization.
Embryo culture involves supporting the fertilized eggs in the laboratory until it is time to transfer them back to the uterus. The dividing embryo has unique nutritional requirements during its different growth periods in the laboratory. Therefore the embryos (and sperm) are exposed to at least 3 different culture media during the IVF process. The embryos may be transferred back into the uterus at anytime after fertilization, however the majority of patients have their embryos transferred 3 days after retrieval and others 5 days after retrieval. Day 5 transfer is usually offered to patients who have many good quality embryos. By waiting to Day 5, embryologists have better opportunities to select the best embryos for transfer. This allows for fewer embryos to be transferred thereby reducing the risk of multiple gestations. Embryos not transferred may be frozen (cryopreserved) for use at a later date.

The developing embryo contains 6-8 cells 3 days after fertilization (picture on the left). Five days after fertilization it is called a blastocyst and has approximately 100 cells (picture on the right).

Embryo biopsy is typically performed 3 days after fertilization. A cell is removed and sent for genetic testing, as shown on the left.
Embryos are transferred back to the uterus using a flexible plastic catheter and ultrasound guidance. The number of embryos transferred depends on a number of prognostic factors in combination with patient preferences. For example, a 37 year old may elect to transfer 2-3 embryos in order to get the best chance at a pregnancy and risk conceiving twins or triplets if all embryos implant. However, if she desires to avoid twins and multiples, a single embryo can be transferred and still maintain a good success rate.
In summary, IVF is a complex process that requires a tailored approach based on patients age, diagnosis and history. It can be successful for many patients.
Frequently Asked Questions:
What are my chances of getting pregnant with IVF?
The success rates for IVF vary widely depending on patients’ characteristics and are between 5 and 50% for most patients. The strongest predictor of success is the female partner’s age. As a woman gets older, her egg quality goes down and the chance of getting pregnant per egg retrieved is lower. In addition, age is a strong predictor of miscarriage as well. Other factors such as infertility diagnosis, ovarian function and endometrial receptivity can affect success rates as well.
What can I do to improve my chances?
Keep trying! Because the odds of success are less than 50%, most patients will have to try more than once in order to achieve success. The two strongest predictors of live birth per cycle are age and ovarian reserve and these cannot be changed. Understanding the cause of infertility is important so that treatment can be tailored to your specific case. In some cases, laparoscopy to remove damaged fallopian tubes or treat endometriosis or hysteroscopy to remove endometrial polyps or scarring can improve your odds of success after a failed attempt.
What can I do to reduce my risk of miscarriage?
The majority of miscarriages are due to sporadic genetic abnormalities. These abnormalities are more common as women get older. Genetic miscarriages cannot be prevented. They are nature’s way of preventing a genetically abnormal conception from progressing. Women, who have had 3 or more consecutive miscarriages, should be evaluated for anatomic, genetic, hematological and hormonal causes or recurrent miscarriages. Treatment strategies for women with unexplained miscarriage due to age include the use of egg donation or preimplantation genetic diagnosis (PGD).

What is implantation and what does it depend on?
A healthy implantation and pregnancy requires a healthy embryo and a healthy endometrium (the lining of the uterus). It is difficult to know the health of an embryo prior to implantation. We know that even embryos that look normal can be either genetically or biochemically abnormal and that poor quality embryos can lead to healthy pregnancies.
How do I know if my uterus in receptive?
During stimulation for IVF the endometrium is monitored. The appearance of the endometrium (thickness and pattern) on ultrasound has been shown to impact success rates. Prior to IVF your doctor should evaluate your uterine cavity for abnormalities with a hysteroscopy, saline ultrasound or HSG. Uterine cavity abnormalities such as polyps or scarring can be treated with hysteroscopy prior to and IVF cycle to improve receptivity.
What is Preimplantation Genetic Diagnosis (PGD)?
PGD is a relatively new technology which allows us to test an egg or embryo for genetic abnormalities prior to embryo transfer. It can be used to diagnose single gene disorders such as cystic fibrosis and thallasemia or chromosomal disorders such as translocations or aneuploidy. Aneuploidy is an abnormal number of chromosomes, which commonly leads to miscarriage or genetic disorders such as Down’s syndrome.
How do I know if I need an egg donor?
If you have tried IVF and failed due to poor embryo quality or quantity your doctor may recommend that you use an egg donor. Age related success rates and miscarriage rates are tied to the age of the egg donor not the recipient. Success rates are over 50% for patients using young egg donors and do not depend on the age of the recipient, as long as she is less than 50 years old. Women with elevated FSH levels or who are over 42 years old having low chances of success using their own eggs for IVF and therefore may consider using an egg donor as a first treatment.
How do I know if I need a gestational carrier/surrogate?
If there are reasons the female partner cannot safely or successfully carry a pregnancy to term, a gestational carrier should be considered. A gestational carrier is a woman who will carry and deliver the baby for the infertile couple. The egg and sperm come from the intended parents and is implanted in the uterus of the gestational carrier. Examples of indications for gestational carrier are; uncorrectable uterine anomalies and medical conditions of the mother which make pregnancy too risky to her health